ABSTRACT
Adequate nutritional intake in elderly individuals improves frailty. Elderly individuals may exhibit improvements in frailty with the use of community care facilities. Therefore, this study evaluated the effects of nutritional intervention in elderly subjects at community care facilities receiving oral nutritional supplements (ONSs) and determined their nutritional status. Sixty-two elderly individuals using community care facilities were divided into the experimental group (EG) (before [n = 31]/after [n = 28]) and control group (CG) (before [n = 31]/after [n = 25]). Subjects in both groups were treated with ONSs (200 mL/200 kcal) for 90 days. However, those in the EG received the product with increased protein; vitamins A, C, D, and E; phosphorus; calcium; and zinc. The data collected included anthropometric data, dietary assessment findings, frailty status (Korean version of the Fatigue, Resistance, Ambulation, Illnesses, and Loss of weight questionnaire), and nutritional status (Mini Nutritional Assessment, MNA). The changes in the two groups were analyzed using the Mann–Whitney U Wilcoxon signed-rank test. Nutritional intervention increased the weight, body mass index, and lean body mass in the EG (p < 0.05). Protein, calcium, and iron levels increased only in the EG (p < 0.05). The MNA score increased and sum of frailty indicators improved in the EG, and the increase in the MNA score in the EG was greater than that in the CG. This study verified the improved anthropometric data and dietary intake in the EG. Thus, the higher number of pre-frailty elderly individuals at facilities of community care indicates the need for adequate nutritional supplementation for frailty management.
-
Keywords: Nutritional support; Frailty; Nutritional status; Randomized controlled trial
INTRODUCTION
Elderly individuals aged 65 years or older accounted for 14.9% of the population in Korea in 2019 [
1], which is continuously increasing, reflecting the trend worldwide. As this trend can lead to social challenges such as increased medical expenses and dependent population, various investigation and management for the welfare of the elderly are needed at the national level. Thus, the government is implementing a long-term elder care system to address the social problems, and facilitate the health care management of the elderly population [
2]. The facilities ensure the activities of daily life for the elderly who require relatively lower levels of care. The objectives of the facilities of community care for the elderly are to delay the decrease in physical function, and to enhance the physical recovery by providing meals and leisure/rehabilitation programs.
The decreased physical function in the elderly is attributed to aging, while the functional challenges are due to frailty [
3]. It is not a simple aging phenomenon, but the loss of functional homeostasis to cope adequately with external stimuli [
4]. Frailty increases the duration of hospitalization in patients sustaining falls and contributes to mortality of the elderly [
5,
6]. Severe frailty requires increased levels of long-term care and management due to decreased physical activities and slow recovery. Thus, decreasing the risk factors underlying frailty in the elderly is very important to enhance their quality of life and health expectancy, and to reduce medical expenses.
Several factors such as age, number of chronic diseases, falls, depression, activities of daily living, and nutritional status affect the progress of frailty [
7,
8,
9]. Nutritional status is related to subjective health status, chronic diseases, type of living (living alone or together with family), social support, and dietary intake [
10,
11,
12,
13]. In particular, dietary intake has the greatest effect on the status of frailty [
14,
15]. Previous studies reported that the intake of total energy, protein, vitamin D, and calcium determined frailty, hospitalization rate, and mortality [
16,
17,
18,
19,
20]. The elderly population consuming enough protein and vitamin D showed improved physical function and increased muscle mass [
21,
22]. An analysis of health conditions based on the intake of calcium, vitamin D, magnesium, and phosphorus, which is associated with musculoskeletal health, showed that the body function scores were significantly low in the group with low intakes of these nutrients [
23]. Zinc and iron are known to be associated with reduced oxidative stress and are likely to be important in preventing muscle loss [
24].
Epidemiological studies and clinical trials have focused on improving the nutritional status of the elderly mainly via single nutrient supplementation. Therefore, studies are needed to elucidate the effects of multiple nutrient supplementations on elderly to improve their nutritional status.
Thus, following the administration of oral nutritional supplement (ONS) including multinutrients to the elderly at the facilities of community care for the elderly, the effects of ONS on the management of frailty were evaluated according to the nutritional status and relevant frailty indicators.
MATERIALS AND METHODS
Subjects and exclusion criteria
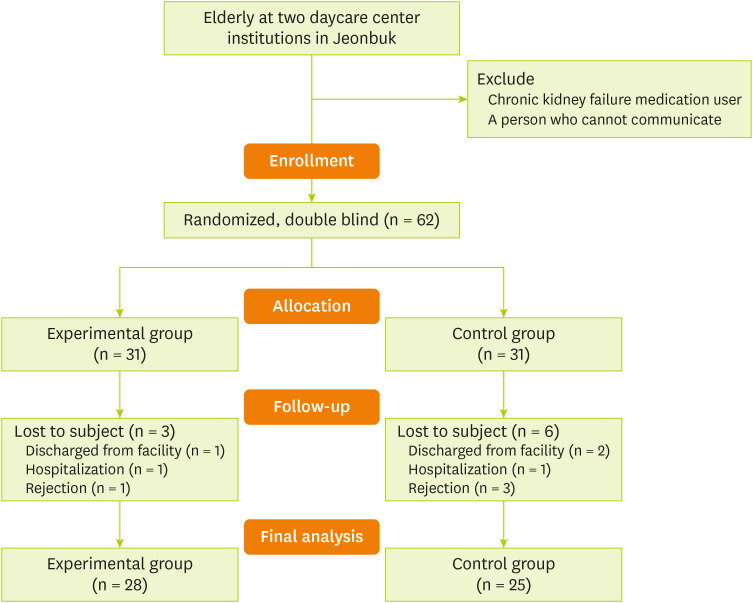
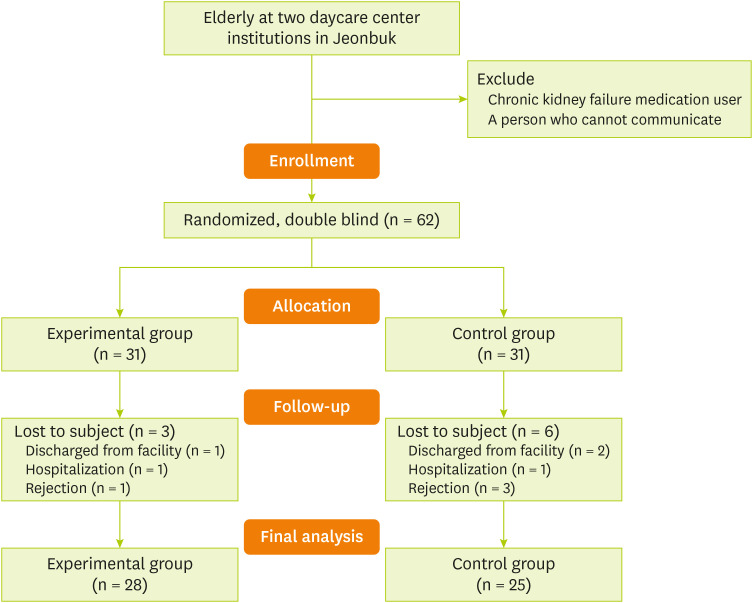
A case-controlled, double-blind, and randomized controlled trial was conducted to evaluate the effects of a multinutrient-ONS. The number of study subjects was determined using the G-power 3.0. A paired t-test at a significance level of 5% and a power of 0.8 based on a 95% confidence interval were used. The total number of subjects was 52 including 26 per group, and the final number of subjects was set at 62 based on a 20% dropout rate. The present study was approved by the Clinical Test Deliberation Commission of Institutional Review Board (IRB), Wonkwang University (WKIRB-201907-HR-057). Subjects were selected based on a 2-week preliminary study starting from August 2019, targeting the elderly at 2 facilities of community care in Jeollabuk-do following informed consent. Anthropometric measurements were conducted. In addition, hand grip, health behavior, and dietary intake were measured. We excluded patients who were treated with medications for chronic renal failure or could not communicate. Finally, the study randomized the 62 elderly subjects to 2 groups of 31 each based on sex and frailty status via stratified cluster random sampling. The number of research participants until the termination of this study included 28 subjects in the experimental group (EG) and 25 subjects in the control group (CG) (
Figure 1).
Figure 1Flow diagram of subject selection.
Nutritional intervention
Composition of ONS and placebo
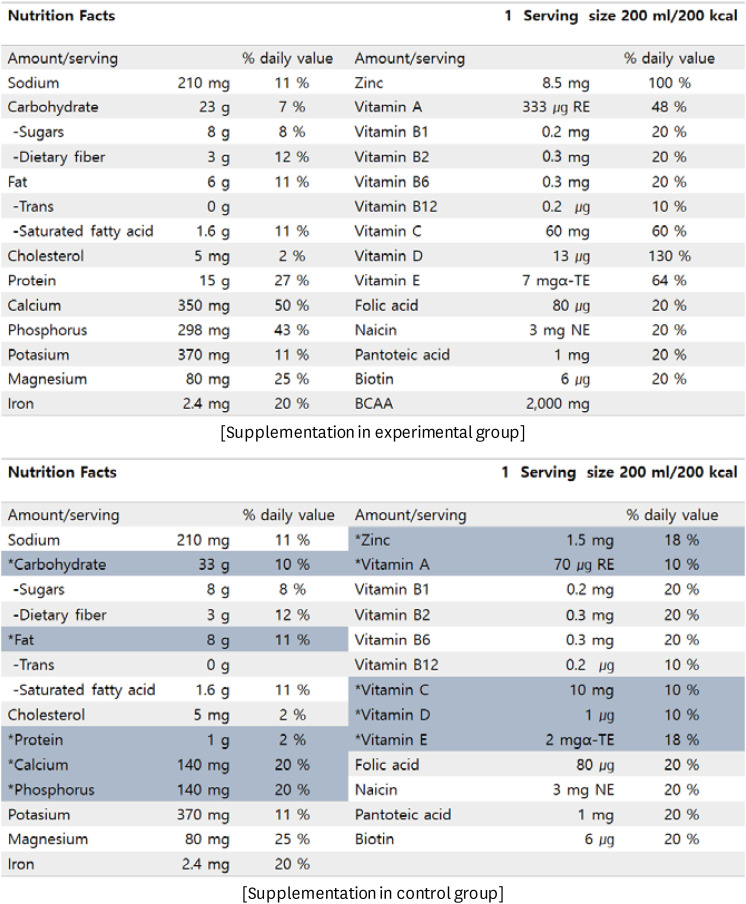
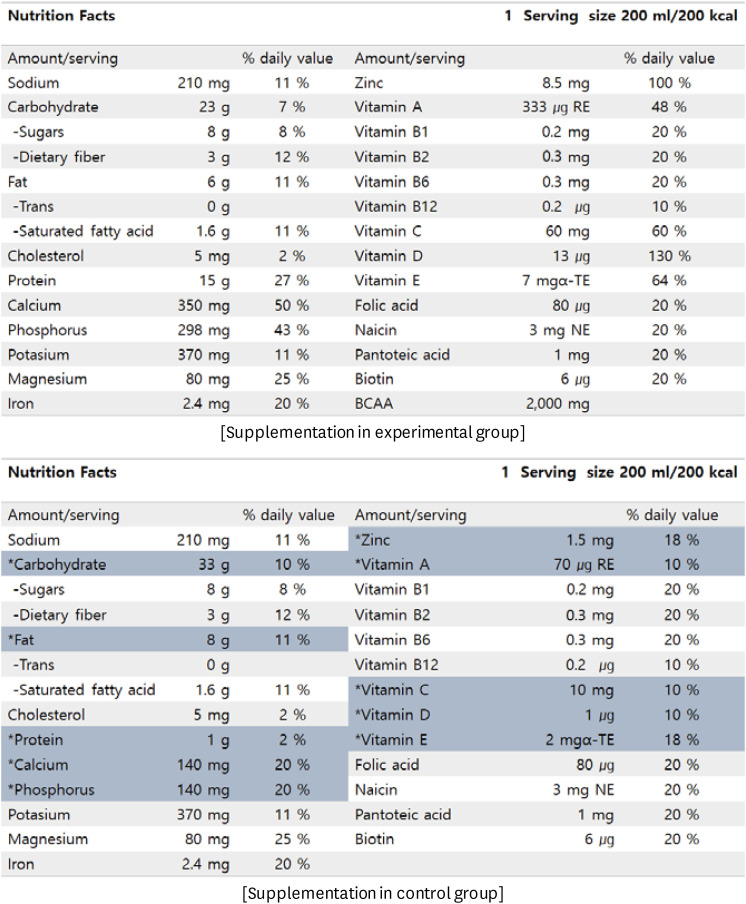
An ONS (200 mL, 200 kcal per day per dose) was provided as a drink made by the manufacturing approved company. Each dose of the ONS administered to the EG contained 15 g of protein, 23 g of carbohydrate, and 6 g of fat. In addition, the ONS contained calcium (daily intake/intake ratio compared with daily recommended calories; 350 mg, 50%), phosphorous (298 mg, 42.5%), zinc (8.5 mg, 94.4%), vitamin A (333 µg RAE, 60.5%), vitamin C (60 mg, 60%), vitamin D (13 µg, 86.7%), and vitamin E (7 mg, 58.3%). Placebo contained the same calorie levels as the ONS. It contained protein 1 g, carbohydrate 33 g, fat 8 g, calcium (140 mg, 20.0%), phosphorus (140 mg, 20.0%), zinc (1.5 mg, 16.7%), vitamin A (70 µg RAE, 12.7%), vitamin C (10 mg, 10%), vitamin D (1 µg, 0.7%), and vitamin E (2 mg, 16.6%). The nutritional supplement was administered for 90 days to each group (
Figure 2).
Figure 2
Nutrient composition of the supplementation.
*Indicated value means nutrients of different amount content in the 2 products.
In this study, ONS was supplied for 90 days. We asked the participating agencies to ensure the same level of meals served during that period. ONS was also served once daily during the morning snack time. In the case of weekends or when participants were off, the center officials provided the ONS in advance. The effect of nutritional supplementation was evaluated as described in “Analysis of Effects” part.
Analysis of effects
Dietary intake
We investigated the dietary intakes using dietary records before and after nutritional intervention. The meal type, mealtime and food quantity were determined. Also, in case of elderly subjects who returned home early, we called their guardians to investigate the meal and food intake at home. The nutrient intake from meal and food was analyzed using CAN-Pro 5.0 (web version).
Anthropometry
All anthropometric measurements were performed in subjects wearing light clothing without shoes and after visiting the toilet. Body weight was measured to the nearest 0.1 kg using a calibrated weighing scale. BMI was calculated as weight (kg) divided by the estimated height in meters squared (m2). The circumference of calf and arm was measured to the nearest 0.1 cm on the left side of the body using a measuring tape. Body composition was measured via bioelectrical impedance analysis (BIA) with Inbody S10 (Inbody, Seoul, Korea).
Physical function
Physical function was measured in terms of handgrip strength using a Hand Dynamometer GRIP-SYS, model DW-781/780 (Deawoo Sports Industry, Seoul, Korea). We measured both hands, each twice, and used the average value. All values were expressed in kg.
Health status
To evaluate the effects of the multi nutrient containing ONS, we evaluated the frailty, health and dietary status of the subjects. The frailty status was determined using the Korean version of the fatigue, resistance, ambulation, illnesses, and loss of weight scale (K-FRAIL) [
25]. The evaluation was based on a total of 5 items such as fatigue, resistance, ambulation, illness and loss of weight. A score of zero meant normal status, 1–2 points suggested pre-frail, and 3–5points indicated frail. In case of illness, chronic disease was indicated by the presence of 5 or more diseases, including hypertension, diabetes, cancer, chronic lung disease, myocardial infarction, heart failure, angina, asthma, arthritis, cerebral infarction, and kidney disease.
The nutritional status was evaluated using the Mini Nutritional Assessment (MNA). The MNA score was based on a total of 18 items such as anthropometry, overall physical/psychological assessment, dietary status, and self-perception of health and nutrition [
26]. Based on the total score of 30, malnutrition was indicated by a score less than 17. The risk of malnutrition was indicated by a score of 17–23.5, whereas scores 24 or higher suggested adequate nourishment. The health status was evaluated using the Korean Activities of Daily Living (K-ADL) instrument [
27] and Korean version of Mini-Mental State Examination (MMSE-K) [
28]. The evaluation of the K-ADL was based on seven items such as getting dressed, washing face, taking a bath, having a meal, moving, using the bathroom, and controlling the bowel and bladder function, and based on the cumulative score complete independence, partial and complete dependence was established. The total score was 21, and a higher score indicated higher dependence. The MMSE-K included a 27 items, including time orientation, place orientation, memory registration, attention/concentration & calculation, memory recall, and composition of language & time-space. The scores were based on sex, age, and level of education according to the user guidelines. The MMSE-K depends on the total score of 30, with a score of 0–19 indicating definite dementia, 20-23 suggesting suspected dementia, and 24-30 considered normal. The appetite assessment questionnaire was evaluated using the Simplified Nutritional Appetite Questionnaire [
29], and the evaluation included 4 items such as appetite, satiety, taste, and the number of meals taken each day. In the total score of 20, a score of 0-14 suggested loss of appetite and a score of 15–20 was considered normal.
The t-test and χ2 test was performed to compare before intervention. And the Wilcoxon signed rank test was performed to validate the changes in both groups after nutritional intervention. In case of non-normal distribution, the Mann-Whitney U test was conducted for comparative analysis. In order to analyze the distribution of frailty diagnosis in the experimental and CGs, the cross-tabulation analysis was conducted. The statistical analysis was conducted using the SPSS version 24.0. The significance level was set at a p < 0.05.
RESULTS
General baseline characteristics
The general characteristics, anthropometry, frailty status, and MNA of the 62 subjects recruited initially are listed in
Table 1. The 62 subjects were divided into an EG (n = 31) and a CG (n = 31). The study included 11 male (17.7%). The average age was 80.8 ± 7.0 years. A normal status was found in 10 (16.1%) subjects, whereas pre-frailty was observed in 45 (72.6%) subjects, and frailty was detected in 7 (11.3%) subjects. The MNA score was 19.8 ± 3.1, suggesting no significant differences between the 2 groups. Data that analyzed only the final subjects before the experiment are presented in
Supplementary Table 1.
Table 1General characteristics at baseline
Table 1
|
Variables |
Total (n = 62) |
Experimental group (n = 31) |
Control group (n = 31) |
p value |
|
Sex (male) |
11 (17.7) |
5 (16.1) |
6 (19.4) |
0.740*
|
|
Age (yr) |
80.8 ± 7.0 |
79.5 ± 7.0 |
82.1 ± 6.9 |
0.143*
|
|
No. of medicine |
4.0 ± 5.1 |
4.5 ± 7.0 |
3.5 ± 1.6 |
0.446*
|
|
Living alone |
16 (25.8) |
9 (29.0) |
7 (22.6) |
0.562†
|
|
Regular exercise |
|
|
|
0.858†
|
|
None |
4 (6.5) |
2 (6.7) |
2 (6.3) |
|
1–3 times/wk |
5 (8.1) |
3 (10.0) |
2 (6.3) |
|
Over 4 times/wk |
53 (85.5) |
25 (83.3) |
28 (87.5) |
|
BMI (kg/m2) |
22.8 ± 3.4 |
23.1 ± 3.7 |
22.4 ± 3.0 |
0.391 |
|
Height (cm) |
153.1 ± 8.6 |
154.0 ± 9.1 |
152.4 ± 8.1 |
0.480 |
|
Weight (kg) |
53.5 ± 9.8 |
55.0 ± 10.7 |
52.1 ± 8.7 |
0.247 |
|
SBP (mmHg) |
125.1 ± 18.7 |
123.4 ± 19.4 |
126.7 ± 18.1 |
0.488 |
|
DBP (mmHg) |
70.7 ± 10.2 |
70.0 ± 10.6 |
71.6 ± 9.9 |
0.588 |
|
Arm circumference (cm) |
27.0 ± 3.2 |
27.2 ± 3.4 |
26.7 ± 3.1 |
0.525 |
|
Calf circumference (cm) |
31.4 ± 3.4 |
32.0 ± 3.5 |
30.9 ± 3.2 |
0.202 |
|
Hand grip (kg) |
12.6 ± 5.8 |
12.7 ± 5.1 |
12.4 ± 6.3 |
0.871 |
|
Frail status |
|
|
|
0.778†
|
|
Normal |
10 (16.1) |
6 (18.8) |
4 (13.3) |
|
Pre-frail |
45 (72.6) |
23 (71.9) |
22 (73.3) |
|
Frail |
7 (11.3) |
3 (9.4) |
4 (13.3) |
|
MNA |
19.8 ± 3.1 |
19.8 ± 3.1 |
19.7 ± 3.2 |
0.953 |
Changes in anthropometry and health status after nutritional intervention
The changes in anthropometry and health status after each nutritional intervention are listed in
Table 2. The final analysis targeted 28 subjects in the EG and 25 subjects in the CG. In the EG, the weight was significantly increased from 56.0 ± 10.3 kg to 57.7 ± 10.1 kg (p = 0.004), while the BMI was also significantly increased from 23.4 ± 3.6 kg/m
2 to 24.1 ± 3.4 kg/m
2 (p = 0.004). The anthropometric values of EG were increased along with a significant increase in the arm and calf circumference, and lean mass. In the CG, the MMSE-K was significantly decreased from 16.1 ± 4.8 to 14.8 ± 5.2 (p = 0.040). Even though no changes were detected in the EG, the cognitive function was diminished in the CG.
Table 2Changes in anthropometry and health status after nutritional intervention
Table 2
|
Variables |
Experimental group (n = 28) |
Control group (n = 25) |
p value‡
|
|
Before |
After |
p value*
|
Mean change from baseline |
Before |
After |
p value†
|
Mean change from baseline |
|
Weight (kg) |
56.0 ± 10.3 |
57.7 ± 10.1 |
0.004 |
1.7 |
51.8 ± 8.6 |
51.8 ± 8.6 |
0.230 |
0.6 |
0.501 |
|
BMI (kg/m2) |
23.4 ± 3.6 |
24.1 ± 3.4 |
0.004 |
0.7 |
22.2 ± 3.1 |
22.7 ± 3.2 |
0.152 |
0.5 |
0.580 |
|
Arm circumference (cm) |
27.5 ± 3.3 |
28.2 ± 2.9 |
0.028 |
0.7 |
26.5 ± 3.1 |
27.3 ± 2.5 |
0.174 |
0.7 |
0.907 |
|
Calf circumference (cm) |
32.4 ± 3.3 |
33.7 ± 3.4 |
0.010 |
1.4 |
30.8 ± 3.3 |
31.6 ± 3.2 |
0.093 |
0.7 |
0.337 |
|
Body fat (%) |
35.0 ± 7.0 |
35.2 ± 7.5 |
0.858 |
0.2 |
34.4 ± 7.1 |
35.0 ± 7.1 |
0.564 |
0.6 |
0.809 |
|
Lean mass (kg) |
36.2 ± 7.1 |
37.3 ± 7.8 |
0.011 |
1.1 |
32.9 ± 4.8 |
31.7 ± 5.2 |
0.051 |
0.8 |
0.603 |
|
Hand grip (kg) |
12.9 ± 5.2 |
13.1 ± 5.5 |
0.790 |
0.2 |
11.9 ± 5.5 |
11.9 ± 4.8 |
0.954 |
0.1 |
0.914 |
|
ASM (kg) |
14.7 ± 4.0 |
14.9 ± 4.1 |
0.183 |
0.2 |
12.6 ± 3.0 |
12.5 ± 2.9 |
0.403 |
−0.1 |
0.122 |
|
ASM/height (kg/m2) |
6.0 ± 1.1 |
6.1 ± 1.1 |
0.154 |
0.1 |
5.4 ± 0.9 |
5.3 ± 0.8 |
0.464 |
−0.0 |
0.127 |
|
ADL |
9.6 ± 2.9 |
9.3 ± 2.4 |
0.450 |
−0.3 |
10.0 ± 3.3 |
9.3 ± 1.9 |
0.311 |
−0.7 |
0.059 |
|
SNAQ |
14.0 ± 1.7 |
14.6 ± 1.6 |
0.165 |
0.6 |
14.6 ± 1.8 |
14.0 ± 1.8 |
0.203 |
−0.6 |
0.258 |
|
MMSE |
15.9 ± 6.1 |
15.7 ± 6.2 |
0.710 |
−0.2 |
16.1 ± 4.8 |
14.8 ± 5.2 |
0.040 |
−1.3 |
0.148 |
Changes in frailty diagnosis and nutritional indicators after intervention
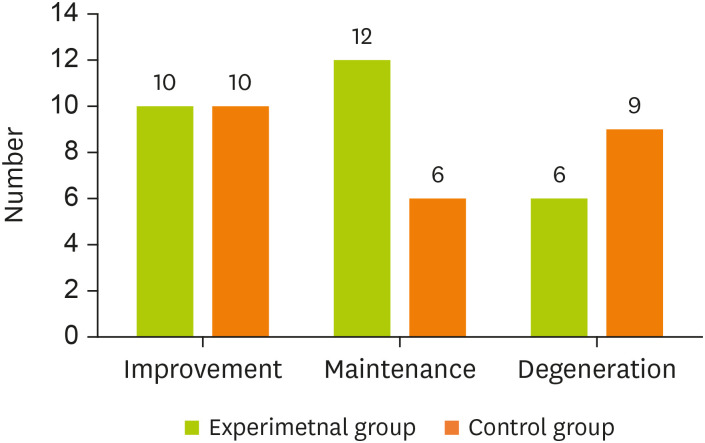
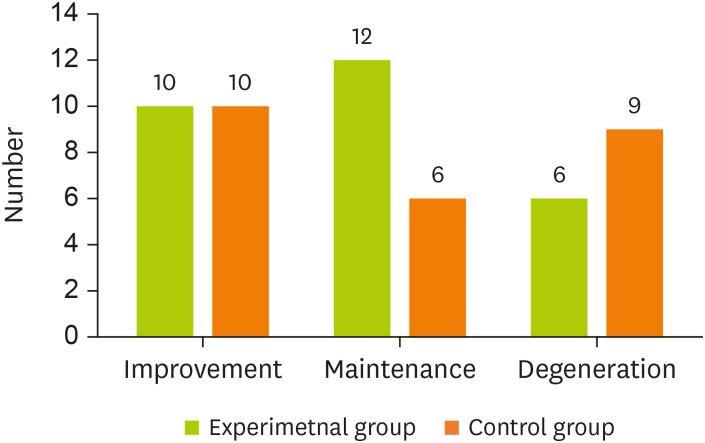
The changes in frailty diagnosis and indicators are listed in
Table 3 and
Figure 3. None of the subjects in the experimental or the CG showed significant differences in frail status. The MNA was changed significantly from 19.7 to 21.1 in the EG (p = 0.004). But MNA was showed no significant differences in the CG (p = 0.900). Based on the sum of frailty indicator (range, 0–5) after nutritional intervention, 10 persons showed improvement in both groups. The subject who remains in the pre-experimental state, were 12 persons in the EG and 6 persons in the CG. The sum of frailty indicators deteriorated in 6 persons in the EG and 9 persons in the CG.
Table 3Changes in frailty status and nutritional status after nutritional intervention
Table 3
|
Variables |
Experimental group (n = 28) |
Control group (n = 25) |
|
Before |
After |
p value |
Before |
After |
p value |
|
Frail status |
|
|
0.549 |
|
|
0.841 |
|
Normal |
7 (25.0) |
10 (35.7) |
4 (16.0) |
5 (20.0) |
|
Pre-frail |
19 (64.9) |
15 (53.6) |
17 (68.0) |
15 (60.0) |
|
Frail |
2 (7.1) |
3 (10.7) |
4 (16.0) |
5 (50.0) |
|
Frail score (total 5) |
1.4 ± 1.0 |
1.2 ± 1.1 |
0.312*
|
1.7 ± 0.9 |
1.6 ± 1.1 |
0.641†
|
|
MNA total score |
19.7 ± 3.0 |
21.1 ± 2.6 |
0.004*
|
19.8 ± 3.2 |
19.7 ± 4.3 |
0.900†
|
Figure 3Comparison of improvement levels through frail parameter after nutrition intervention. The bars and digits indicate that the level of sum of frail parameter score. Changes of improvement levels though sum of frail parameter before and after the nutrition intervention were compared between control group and experimental group.
Changes in dietary intake after nutritional intervention
The changes in dietary intake after nutritional intervention are shown in
Table 4. Even though no changes were detected in the CG, the nutrient levels were slightly increased in the EG. In case of dietary intake, the levels of energy, carbohydrate, dietary fiber, vitamin A, vitamin K, vitamin C, thiamine, riboflavin, and vitamin B6 were significantly increased in both groups. However, the levels of protein, calcium, and iron intakes were increased only in the EG.
Table 4Changes in dietary intake after nutritional intervention
Table 4
|
Variables |
Experimental group (n = 28) |
Control group (n = 25) |
p value‡
|
|
Before |
After |
p value*
|
Mean change from baseline |
Before |
After |
p value†
|
Mean change from baseline |
|
Energy (kcal) |
1,311.6 ± 192.9 |
1,479.6 ± 339.2 |
0.031 |
168.0 |
1,259.0 ± 226.0 |
1,402.1 ± 280.2 |
0.002 |
143.1 |
0.769 |
|
Carbohydrate (g) |
207.9 ± 29.3 |
235.3 ± 40.0 |
0.006 |
27.4 |
202.9 ± 28.3 |
228.3 ± 36.3 |
0.001 |
25.3 |
0.849 |
|
Fat (g) |
33.0 ± 6.7 |
30.7 ± 13.3 |
0.390 |
−2.3 |
30.7 ± 10.0 |
33.3 ± 12.7 |
0.233 |
2.6 |
0.157 |
|
Protein (g) |
43.7 ± 8.6 |
62.1 ± 19.4 |
0.000 |
18.4 |
41.4 ± 10.9 |
44.0 ± 15.0 |
0.315 |
2.6 |
0.003 |
|
Protein (g/kg)§
|
0.8 ± 0.2 |
1.1 ± 0.3 |
0.000 |
0.30 |
0.9 ± 0.3 |
0.9 ± 0.4 |
0.449 |
0.04 |
0.004 |
|
Fiber (g) |
15.5 ± 3.5 |
20.7 ± 7.0 |
0.001 |
5.3 |
16.0 ± 4.6 |
19.5 ± 5.9 |
0.002 |
3.5 |
0.325 |
|
Vitamin A (ug RAE) |
415.2 ± 168.0 |
1,169.7 ± 387.7 |
0.000 |
754.4 |
392.7 ± 191.9 |
806.6 ± 304.3 |
0.000 |
413.9 |
0.004 |
|
Vitamin D (ug) |
0.8 ± 0.8 |
13.5 ± 0.5 |
0.000 |
12.7 |
1.0 ± 1.1 |
1.4 ± 0.5 |
0.131 |
0.4 |
0.000 |
|
Vitamin E (mg) |
16.1 ± 3.5 |
17.6 ± 7.5 |
0.390 |
1.5 |
14.5 ± 5.4 |
13.5 ± 6.3 |
0.568 |
−1.0 |
0.308 |
|
Vitamin K (ug) |
77.3 ± 84.4 |
245.7 ± 148.5 |
0.001 |
168.3 |
75.1 ± 69.2 |
228.0 ± 100.4 |
0.000 |
152.9 |
0.766 |
|
Vitamin C (mg) |
29.4 ± 12.5 |
103.5 ± 15.2 |
0.000 |
74.1 |
27.1 ± 13.6 |
49.2 ± 16.5 |
0.000 |
22.1 |
0.000 |
|
Thiamin (mg) |
1.0 ± 0.2 |
1.3 ± 0.4 |
0.004 |
0.3 |
0.9 ± 0.3 |
1.2 ± 0.4 |
0.000 |
0.3 |
0.892 |
|
Riboflavin (mg) |
0.8 ± 0.2 |
0.9 ± 0.3 |
0.017 |
0.2 |
0.8 ± 0.3 |
1.0 ± 0.2 |
0.000 |
0.2 |
0.490 |
|
Niacin (mg) |
7.7 ± 1.8 |
7.8 ± 2.3 |
0.880 |
0.1 |
7.5 ± 1.9 |
7.3 ± 2.2 |
0.761 |
−0.1 |
0.753 |
|
Vitamin B6 (mg) |
0.8 ± 0.2 |
1.2 ± 0.3 |
0.000 |
0.4 |
0.7 ± 0.2 |
1.1 ± 0.3 |
0.000 |
0.4 |
0.901 |
|
Folate (ug) |
242.1 ± 88.3 |
218.7 ± 60.0 |
0.280 |
−23.5 |
241.4 ± 88.6 |
201.6 ± 64.8 |
0.024 |
−39.8 |
0.547 |
|
Vitamin B12 (ug) |
2.9 ± 2.7 |
4.6 ± 3.0 |
0.003 |
1.8 |
3.3 ± 2.4 |
4.4 ± 2.7 |
0.184 |
1.1 |
0.516 |
|
Calcium (mg) |
409.6 ± 175.7 |
671.3 ± 73.4 |
0.000 |
261.7 |
401.7 ± 195.4 |
439.8 ± 85.9 |
0.405 |
38.1 |
0.001 |
|
Sodium (mg) |
3,207.8 ± 897.2 |
3,650.7 ± 1,097.9 |
0.051 |
442.9 |
2,939.2 ± 676.7 |
3,197.6 ± 904.7 |
0.214 |
258.4 |
0.533 |
|
Phosphorus (mg) |
540.9 ± 202.4 |
949.5 ± 234.5 |
0.000 |
408.6 |
540.4 ± 226.4 |
663.4 ± 185.9 |
0.005 |
112.9 |
0.001 |
|
Zinc (mg) |
4.4 ± 1.4 |
14.2 ± 2.1 |
0.000 |
9.7 |
4.3 ± 1.6 |
5.5 ± 1.6 |
0.000 |
1.2 |
0.005 |
|
Iron (mg) |
11.6 ± 3.2 |
13.8 ± 3.9 |
0.012 |
2.2 |
11.5 ± 3.6 |
12.6 ± 2.9 |
0.127 |
1.1 |
0.290 |
DISCUSSION
In order to evaluate the effects of ONS on the management of frailty in the elderly using facilities of community care for the elderly, nutritional intervention was performed for 90 days and resulted in a significant improvement in anthropometric parameters and dietary intake in the EG.
The MNA score was 19.8 in the elderly subjects at facilities of community care. According to the national survey of the elderly with dementia, the MNA was 17.9, which suggested a relatively higher nutritional status of study subjects. Also, compared with the normal group comprising 16.1% frail subjects, pre-frail was detected in 72.6% and frail in 11.3% (average age, 80.8), suggesting that most of the subjects were diagnosed with pre-frailty. In a study of community-based frailty cohort (Aging Study of Pyeongchang Rural Area), however, normal (29.3%), pre-frail (43.2%), and frail (27.5%) subjects were found (average age, 74.4 years) [
30], suggesting that the distribution based on frailty status of other study differed slightly from this study. The study subjects showed a relatively low distribution in the normal and frail groups, probably because of fewer subjects in the normal category as their age was higher than in other studies. Also, this study only targeted the elderly in facilities of community care as their health status was relatively good without the need for transfer to nursing hospitals. Thus, based on the comparison of the current and the previous studies, the differences in health status of the elderly depended on their residence. Therefore, the elderly who exhibited potential for improvement were densely distributed in the facilities of community care, which delayed the changes in their health status, suggesting the need for concrete nutritional management.
The comparison of dietary intake and nutritional status of experimental and CGs after ONS intervention showed that the intake of protein, vitamin A, vitamin D, vitamin C, and calcium was significantly increased in the EG. In the meta-analysis by Milne et al. [
31], the complications and mortality among malnourished elderly subjects were reduced by treatment with ONS. In this study, the intake per weight was increased from 0.7 to 1.1 g in the EG. In the study by Campbell et al. [
32], the intake of 0.8 g per weight increased the excretion of urinary nitrogen. Due to the catabolism of muscle protein, it is essential to ensure adequate protein intake in the elderly. Thus, the intake of protein supplement in this study is regarded as appropriate for the study subjects. In the analysis of before and after nutritional status, the supplementary protein intake was increased from 19.7 to 21.1 g in the EG, while it was decreased from 19.8 to 19.7 g in the CG. In the study by Pedro, 91 elderly persons were exposed to nutritional supplementation and exercise for 12 weeks, and their nutritional status was evaluated [
33]. The nutritional status was improved after the intervention. Jukkola et al. [
34] conducted a case-control study by providing beverages and food as nutritional supplements to hospitalized patients, which resulted in no significant differences between the 2 groups. Thus, the differences in the results of each study might be attributed to differences based on community, facilities of community care, and hospitalization in the elderly. The number of subjects varied as well, which may have resulted in differences in the improvement of nutritional status between groups.
The results of this study showed that weight, BMI, arm circumference, calf circumference, and lean body mass were significantly increased in the EG, but not in the CG. Payette et al. [
35] reported that treatment of the elderly in the community with protein-energy supplement and nutrient intake through food, resulted in weight increase in the EG and, the observation was similar to this study.
The effects of ONS treatment in the elderly yielded significant results based on physical function, such as Short Physical Performance Battery, Timed Up-and-Go test and handgrip [
33,
36]. However, no significant differences between the 2 groups were detected in the case of handgrip test evaluating physical function index in this study.
In summary, there are several implications based on research subjects and study design. First, this study evaluated nutritional intervention by administering the ONS only for 90 days. Even though this intervention simply changed the anthropometric parameters such as weight or muscle mass in the elderly, the effects on improvement of physical function are insignificant. Previous studies showed improvement in physical function because nutrition was combined with exercise intervention. Therefore, nutritional management programs for delaying frailty would need to include an exercise component.
In the analysis of cognitive function, activities of daily living, and appetite, the changes in physical function and health status were analyzed via nutritional intervention, even though the study subjects were elderly with diminished cognitive function. The MMSE decreased by about 0.2 point in the EG during the nutritional intervention but decreased by 1.3 points in the CG. Even though no significant differences occurred between the 2 groups, considering the elderly with continuous and progressive aging, it is necessary to conduct a follow-up evaluation of the effects on cognitive function via long-term intake.
However, this study has several limitations. In case of dietary intake measurements conducted before and after the study, the estimated data were adjusted for actual intake by the elderly subjects at DC centers. Even though the study is significant in reflecting the actual intake, it may differ from the usual dietary intake. The subjects were recruited via convenient sampling in selected areas, and therefore it is difficult to generalize the findings for all elderly subjects using the facilities of community care for the elderly.
Nevertheless, this study is valuable as a randomized controlled trial which investigated the elderly using facilities of community care in improving their nutritional status and management of frailty. This study evaluated the effects of nutritional intervention using ONS, although the data have not been validated at the community level in Korea. It showed improvement in anthropometric parameters (physical status) and dietary intake. The study targeted individuals in need of relatively low level of care due to their activities of daily living, and low risk of illness. Therefore, given the increasing elderly population in Korea, it will be necessary to conduct a specialized nutritional management program at facilities of community care in the future.
NOTES
-
Conflict of Interest: The authors declare that they have no competing interests.
ACKNOWLEDGEMENTS
NOS-NPO® and Placebo product were provided by Deasang Corporation, Korea.
SUPPLEMENTARY MATERIAL
Supplementary Table 1
General characteristics of final subjects who conducted nutrition intervention
cnr-10-24-s001.xls
REFERENCES
- 1. Statistics Korea. Available from http://kostat.go.kr/portal/korea/index.action
- 2. Hyun EY, Oh JJ. Malnutritional status and it's related factors of demented elderly in long-term care facilities. J Korea Contents Assoc 2017;17:426-436.
- 3. Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, Seeman T, Tracy R, Kop WJ, Burke G, McBurnie MA. Cardiovascular Health Study Collaborative Research Group. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci 2001;56:M146-56.
- 4. Won CW. Evaluation and management of frailty. J Korean Med Assoc 2017;60:314-320.
- 5. Walston J, Hadley EC, Ferrucci L, Guralnik JM, Newman AB, Studenski SA, Ershler WB, Harris T, Fried LP. Research agenda for frailty in older adults: toward a better understanding of physiology and etiology: summary from the American Geriatrics Society/National Institute on Aging Research Conference on Frailty in Older Adults. J Am Geriatr Soc 2006;54:991-1001.
- 6. Cawthon PM, Marshall LM, Michael Y, Dam TT, Ensrud KE, Barrett-Connor E, Orwoll ES. Osteoporotic Fractures in Men Research Group. Frailty in older men: prevalence, progression, and relationship with mortality. J Am Geriatr Soc 2007;55:1216-1223.
- 7. Fhon JR, Rodrigues RA, Santos JL, Diniz MA, Santos EB, Almeida VC, Giacomini SB. Factors associated with frailty in older adults: a longitudinal study. Rev Saude Publica 2018;52:74.
- 8. Arakawa Martins B, Visvanathan R, Barrie H, Huang CH, Matsushita E, Okada K, Satake S, Uno C, Kuzuya M. Frailty prevalence using Frailty Index, associated factors and level of agreement among frailty tools in a cohort of Japanese older adults. Arch Gerontol Geriatr 2019;84:103908.
- 9. Wei K, Nyunt MS, Gao Q, Wee SL, Ng TP. Frailty and malnutrition: related and distinct syndrome prevalence and association among community-dwelling older adults: Singapore longitudinal ageing studies. J Am Med Dir Assoc 2017;18:1019-1028.
- 10. Shlisky J, Bloom DE, Beaudreault AR, Tucker KL, Keller HH, Freund-Levi Y, Fielding RA, Cheng FW, Jensen GL, Wu D, Meydani SN. Nutritional considerations for healthy aging and reduction in age-related chronic disease. Adv Nutr 2017;8:17-26.
- 11. Chang SF, Lin PL. Prefrailty in community-dwelling older adults is associated with nutrition status. J Clin Nurs 2016;25:424-433.
- 12. Luger E, Dorner TE, Haider S, Kapan A, Lackinger C, Schindler K. Effects of a home-based and volunteer-administered physical training, nutritional, and social support program on malnutrition and frailty in older persons: a randomized controlled trial. J Am Med Dir Assoc 2016;17:671.e9-671.e16.
- 13. de Andrade FB, de França Caldas A Jr, Kitoko PM. Relationship between oral health, nutrient intake and nutritional status in a sample of Brazilian elderly people. Gerodontology 2009;26:40-45.
- 14. Leslie WS. Improving the dietary intake of frail older people. Proc Nutr Soc 2011;70:263-267.
- 15. Bernstein MA, Tucker KL, Ryan ND, O’Neill EF, Clements KM, Nelson ME, Evans WJ, Fiatarone Singh MA. Higher dietary variety is associated with better nutritional status in frail elderly people. J Am Diet Assoc 2002;102:1096-1104.
- 16. Omura T, Tamura Y, Yamaoka T, Yoshimura Y, Sakurai T, Umegaki H, Kamada C, Iimuro S, Ohashi Y, Ito H, Araki A. Japanese Elderly Diabetes Intervention Trial Research Group. Assessing the association between optimal energy intake and all-cause mortality in older patients with diabetes mellitus using the Japanese Elderly Diabetes Intervention Trial. Geriatr Gerontol Int 2020;20:59-65.
- 17. McCarty MF, DiNicolantonio JJ. An increased need for dietary cysteine in support of glutathione synthesis may underlie the increased risk for mortality associated with low protein intake in the elderly. Age (Dordr) 2015;37:96.
- 18. Johansson H, Odén A, Kanis J, McCloskey E, Lorentzon M, Ljunggren Ö, Karlsson MK, Thorsby PM, Tivesten Å, Barrett-Connor E, Ohlsson C, Mellström D. Low serum vitamin D is associated with increased mortality in elderly men: MrOS Sweden. Osteoporos Int 2012;23:991-999.
- 19. Tieland M, Brouwer-Brolsma EM, Nienaber-Rousseau C, van Loon LJ, De Groot LC. Low vitamin D status is associated with reduced muscle mass and impaired physical performance in frail elderly people. Eur J Clin Nutr 2013;67:1050-1055.
- 20. Sullivan DH, Bopp MM, Roberson PK. Protein-energy undernutrition and life-threatening complications among the hospitalized elderly. J Gen Intern Med 2002;17:923-932.
- 21. Rondanelli M, Klersy C, Terracol G, Talluri J, Maugeri R, Guido D, Faliva MA, Solerte BS, Fioravanti M, Lukaski H, Perna S. Whey protein, amino acids, and vitamin D supplementation with physical activity increases fat-free mass and strength, functionality, and quality of life and decreases inflammation in sarcopenic elderly. Am J Clin Nutr 2016;103:830-840.
- 22. Isanejad M, Mursu J, Sirola J, Kröger H, Rikkonen T, Tuppurainen M, Erkkilä AT. Dietary protein intake is associated with better physical function and muscle strength among elderly women. Br J Nutr 2016;115:1281-1291.
- 23. Sharkey JR, Giuliani C, Haines PS, Branch LG, Busby-Whitehead J, Zohoori N. Summary measure of dietary musculoskeletal nutrient (calcium, vitamin D, magnesium, and phosphorus) intakes is associated with lower-extremity physical performance in homebound elderly men and women. Am J Clin Nutr 2003;77:847-856.
- 24. Prasad AS. Zinc is an antioxidant and anti-inflammatory agent: its role in human health. Front Nutr 2014;1:14.
- 25. Jung HW, Yoo HJ, Park SY, Kim SW, Choi JY, Yoon SJ, Kim CH, Kim KI. The Korean version of the FRAIL scale: clinical feasibility and validity of assessing the frailty status of Korean elderly. Korean J Intern Med 2016;31:594-600.
- 26. Guigoz Y, Vellas BJ. Malnutrition in the elderly: the Mini Nutritional Assessment (MNA). Ther Umsch 1997;54:345-350.
- 27. Won CW, Rho YG, Kim SY, Cho BR, Lee YS. The validity and reliability of Korean activities of daily living (K-ADL) scale. J Korean Geriatr Soc 2002;6:98-106.
- 28. Kwon YC, Park JH. Korean version of mini-mental state examination (MMSE-K). J Korean Neuropsychiatr Assoc 1989;1:123-135.
- 29. Kruizenga HM, Seidell JC, de Vet HC, Wierdsma NJ, van Bokhorst-de van der Schueren MA. Development and validation of a hospital screening tool for malnutrition: the short nutritional assessment questionnaire (SNAQ). Clin Nutr 2005;24:75-82.
- 30. Jung HW, Jang IY, Lee YS, Lee CK, Cho EI, Kang WY, Chae JH, Lee EJ, Kim DH. Prevalence of frailty and aging-related health conditions in older Koreans in rural communities: a cross-sectional analysis of the aging study of Pyeongchang rural area. J Korean Med Sci 2016;31:345-352.
- 31. Milne AC, Avenell A, Potter J. Meta-analysis: protein and energy supplementation in older people. Ann Intern Med 2006;144:37-48.
- 32. Campbell WW, Trappe TA, Wolfe RR, Evans WJ. The recommended dietary allowance for protein may not be adequate for older people to maintain skeletal muscle. J Gerontol A Biol Sci Med Sci 2001;56:M373-80.
- 33. Abizanda P, López MD, García VP, Estrella JD, da Silva González Á, Vilardell NB, Torres KA. Effects of an oral nutritional supplementation plus physical exercise intervention on the physical function, nutritional status, and quality of life in frail institutionalized older adults: the ACTIVNES study. J Am Med Dir Assoc 2015;16:439.e9-439.e16.
- 34. Jukkola K, MacLennan P. Improving the efficacy of nutritional supplementation in the hospitalised elderly. Australas J Ageing 2005;24:119-124.
- 35. Payette H, Boutier V, Coulombe C, Gray-Donald K. Benefits of nutritional supplementation in free-living, frail, undernourished elderly people: a prospective randomized community trial. J Am Diet Assoc 2002;102:1088-1095.
- 36. Kim H, Suzuki T, Kim M, Kojima N, Ota N, Shimotoyodome A, Hase T, Hosoi E, Yoshida H. Effects of exercise and milk fat globule membrane (MFGM) supplementation on body composition, physical function, and hematological parameters in community-dwelling frail Japanese women: a randomized double blind, placebo-controlled, follow-up trial. PLoS One 2015;10:e0116256.