ABSTRACT
Postgastrectomy diarrhea is often attributed to dumping syndrome or functional changes; however, exocrine pancreatic insufficiency (EPI) from anatomical and physiological alterations may be an underrecognized cause of malabsorption and nutritional decline. Because EPI symptoms are often nonspecific, it may remain undiagnosed and lead to progressive malnutrition if untreated. This case report describes severe EPI identified via nutrition-focused assessment in a patient with persistent diarrhea after Billroth II gastrectomy, and the clinical response to pancreatic enzyme replacement therapy (PERT). A patient with a history of subtotal gastrectomy with Billroth II reconstruction for gastric cancer presented with chronic diarrhea, steatorrhea, weight loss, and hypoalbuminemia. Repeated endoscopic and radiologic evaluations identified no structural cause of diarrhea. Comprehensive nutrition-focused assessment indicated fat malabsorption, and fecal pancreatic elastase was markedly reduced (23.8 µg/g), confirming severe EPI. PERT with pancreatin containing 25,000 units of lipase (Norzyme) was initiated with meals. Posttreatment, steatorrhea resolved and bowel movements normalized without dietary fat restriction. Serum albumin levels subsequently normalized, and body weight returned to the normal range, indicating improved nutritional status. This case emphasizes the clinical value of nutrition-focused assessment in identifying treatable causes of malabsorption, such as EPI, in patients with persistent postgastrectomy diarrhea.
-
Keywords: Exocrine pancreatic insufficiency; Gastrectomy; Pancreatic enzyme replacement therapy; Nutrition therapy; Case reports
INTRODUCTION
With improved survival after gastric cancer surgery, long-term gastrointestinal dysfunction and nutritional complications are increasingly recognized as clinically important. Exocrine pancreatic insufficiency (EPI) has traditionally been associated with pancreatic disease or surgery; however, it is increasingly recognized as a possible complication of gastrointestinal surgery [
1-
6]. Postgastrectomy diarrhea is often attributed to dumping syndrome or functional changes, but EPI with fat malabsorption may be an important cause in some patients.
EPI can cause diarrhea, steatorrhea, abdominal discomfort, malnutrition, and reduced quality of life. However, symptoms are often nonspecific, sometimes mild, and may vary in severity depending on dietary fat intake. Consequently, diagnosis may be easily overlooked or delayed [
2,
7-
10]. If untreated, EPI can worsen nutritional deficiencies and is associated with increased morbidity and mortality [
8,
9].
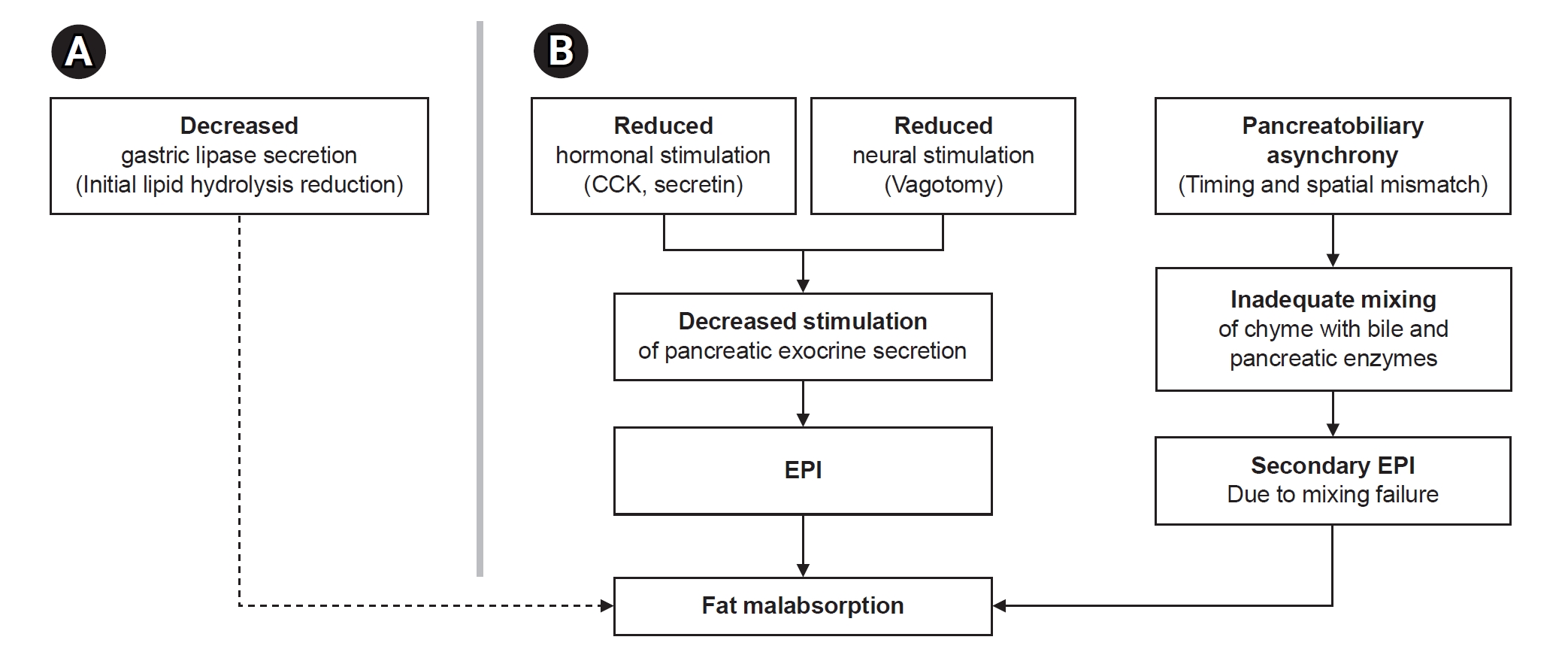
Gastrectomy reduces gastric lipase, which normally contributes approximately 10% to 30% of lipid digestion [
11]. In addition, even without direct pancreatic tissue loss, anatomical changes may reduce hormonal and neural stimulation of pancreatic secretion [
3,
5,
6]. Previous studies reported variable declines in exocrine pancreatic function after gastrectomy, with reductions of up to 76% [
5]. Furthermore, pancreatobiliary asynchrony—mismatch between pancreatobiliary secretions and food transit after Billroth II or Roux-en-Y reconstruction—may further worsen fat malabsorption [
1,
3,
4,
6]. These mechanisms are illustrated in
Fig. 1.
Therefore, early recognition of EPI in patients presenting with postgastrectomy diarrhea, followed by timely nutritional intervention and pancreatic enzyme replacement therapy (PERT), may improve nutritional status, alleviate symptoms, and enhance overall clinical outcomes.
This case report describes a patient with persistent post-Billroth II diarrhea in whom EPI was identified and successfully managed with nutritional intervention and pancreatic enzyme supplementation.
Ethics statement
Ethical approval was obtained from the Institutional Review Board of Seoul National University Hospital (No. H-2603-020-1722). Written informed consent for publication of the research details was obtained from the patient. All study procedures were conducted in accordance with the principles of the Declaration of Helsinki. This study is reported in accordance with the CARE guidelines.
CASE REPORT
Patient information
In 2019, a 49-year-old male patient was referred for evaluation of persistent diarrhea. He had undergone a subtotal gastrectomy with Billroth II reconstruction for advanced gastric cancer in December 2009. Over the preceding 1 to 2 years, he had developed persistent diarrhea with steatorrhea. Prior evaluations at another hospital, including esophagogastroduodenoscopy (EGD), colonoscopy, and abdominal computed tomography, did not identify a cause of his symptoms. Despite symptomatic treatment, his diarrhea persisted, and he was referred to our hospital for further evaluation.
He had no history of chronic illness or other conditions that could account for the weight loss. After transfer, he was started on loperamide (2 mg twice daily); however, diarrhea with steatorrhea persisted more than 4 to 5 times daily. He was admitted for supportive care due to persistent diarrhea, poor oral intake, and weight loss. The patient also reported 3 to 4 episodes of glossitis over the previous year, which made it difficult to tolerate spicy foods. He further complained of facial and extremity edema upon waking.
He was 177 cm tall, with a preoperative body weight of 55 kg (body mass index [BMI], 17.6 kg/m²). Over the preceding 6 months, he had lost approximately 5 kg from his usual postgastrectomy weight of 57 to 58 kg. His body weight was 52.9 kg (BMI, 16.9 kg/m²) on admission, which further decreased to 49.15 kg (BMI, 15.7 kg/m²) during hospitalization.
Dietary and bowel habit assessments showed that his bowel movements were relatively normal with low-fat, non-greasy foods. However, steatorrhea and diarrhea occurred after overeating or consuming high-fat foods, such as fried dishes or oily soups. His stool was typically pale or watery with yellowish fat droplets. Due to sudden urgency and risk of fecal incontinence, he required absorbent pads. During hospitalization, repeat EGD, abdominal radiography (erect), and stool examinations, including parasite tests and fecal calprotectin, did not identify a definitive cause of diarrhea.
Nutritional assessment and diagnosis
On hospital day 4, the patient was referred to a clinical dietitian for counseling to manage steatorrhea-associated diarrhea and prevent dehydration. Based on dietary history, bowel patterns, and history of gastrectomy, EPI with fat malabsorption post-Billroth II gastrectomy was strongly suspected.
Hypoalbuminemia was also considered a contributing factor to intestinal mucosal edema and diarrhea, warranting active nutritional management. A fecal pancreatic elastase test showed a level of 23.8 µg/g, consistent with severe EPI. Trace element testing revealed deficiencies in selenium, zinc, and copper (37.2, 19.3, and 40.8 µg/dL, respectively).
Nutritional intervention and clinical course
Given the patient’s Billroth II reconstruction, pancreatin containing 25,000 units of lipase per meal (Norzyme) was administered with meals as opened capsules. Although coadministration with acidic foods such as orange juice was considered if the response was inadequate, marked improvement occurred even when taken with water.
The previously prescribed low-fat diet was discontinued, and the patient was encouraged to follow a regular diet, providing approximately 30% of total energy from fat. To prevent dumping syndrome, previous dietary advice was reinforced, including avoiding large fluid intake during and immediately after meals, and multivitamin and multimineral supplementation was initiated for micronutrient deficiencies.
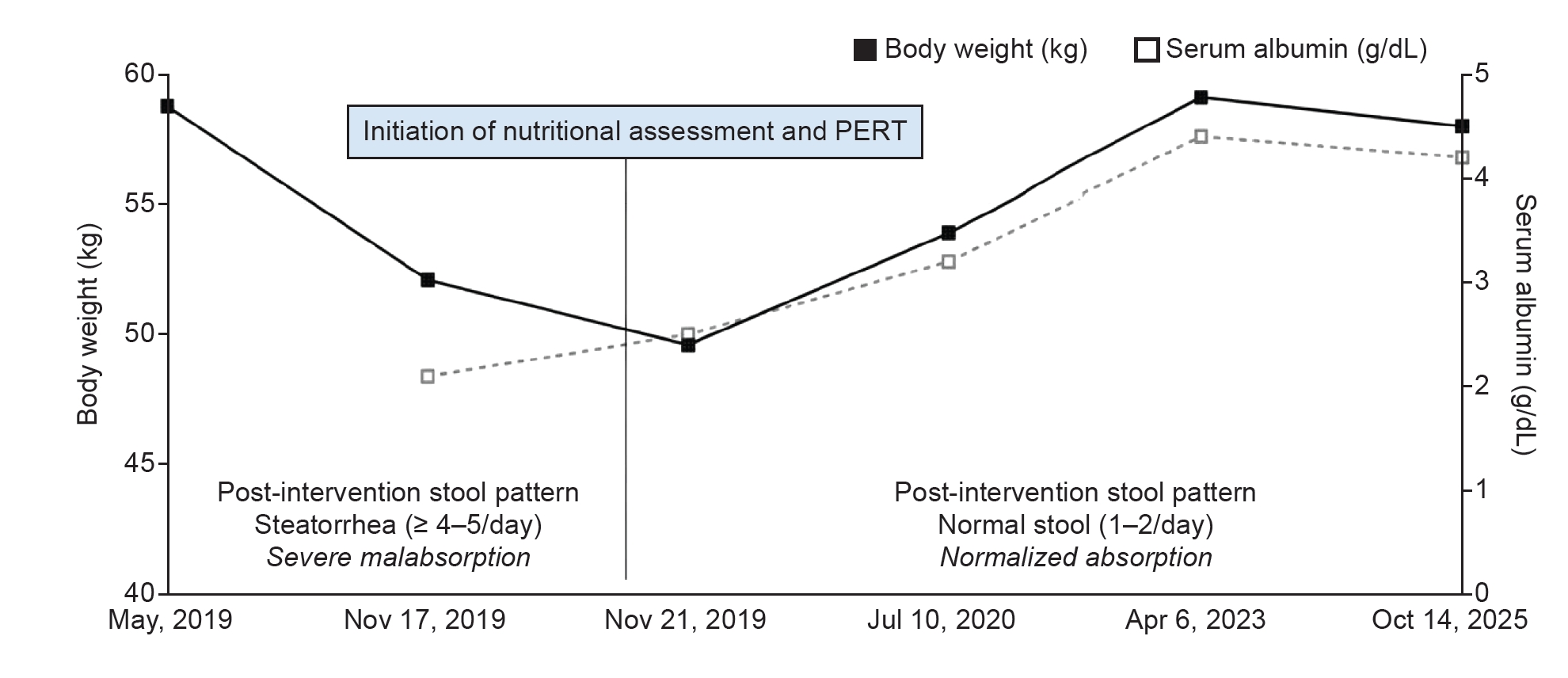
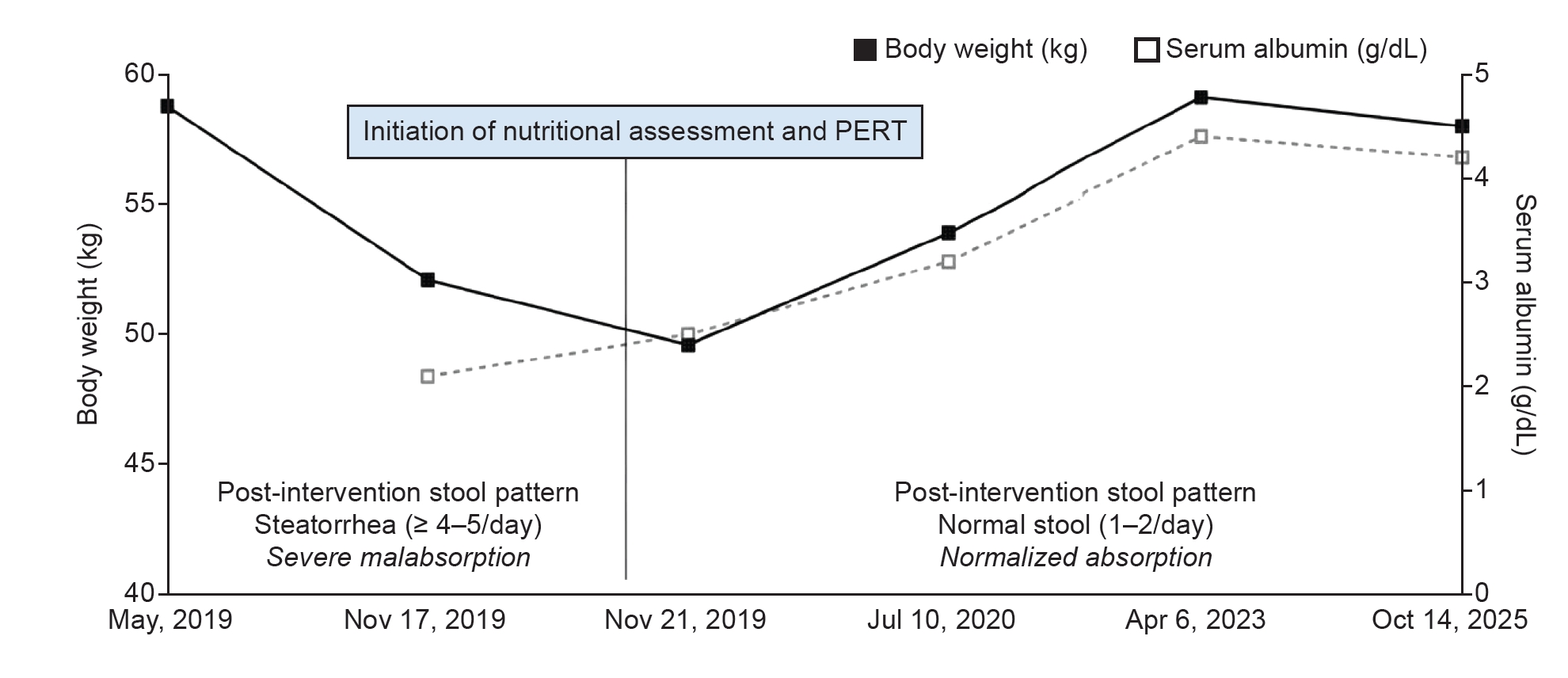
After starting PERT, stool consistency rapidly normalized, steatorrhea improved, bowel movement frequency decreased, and stool color returned to normal. With improved fat malabsorption, serum albumin levels gradually increased, and body weight recovered.
At outpatient follow-up in October 2025, the patient tolerated a regular diet without significant gastrointestinal symptoms. Serum albumin remained within the normal range, and body weight had increased to 58 kg (BMI, 18.5 kg/m²) (
Fig. 2).
DISCUSSION
Postgastrectomy diarrhea is common but often attributed to dumping syndrome or nonspecific postoperative bowel dysfunction and managed empirically. This case is notable because a patient with long-standing post-Billroth II diarrhea and weight loss had no identifiable cause despite repeated imaging and endoscopic evaluations and did not respond to antidiarrheal medication. EPI was suspected during nutrition-focused assessment, confirmed by fecal elastase testing, and successfully treated with PERT. These findings reveal that persistent diarrhea with steatorrhea post-Billroth II gastrectomy may be considered a clinical indicator of EPI. Fat malabsorption occurring a decade after surgery may partly reflect age-related decline in pancreatic exocrine function [
12]. In this context, age-related decline in function may also contribute to symptom exacerbation. Diarrhea-related malabsorption is often overlooked in clinical practice but can significantly impair nutritional status and clinical outcomes through substantial loss of energy and nutrients. Selenium, zinc, and copper deficiencies observed in this patient may also reflect chronic malabsorption due to EPI.
Several studies have investigated nutrient losses associated with diarrhea. One study reported that when daily stool output exceeds 350 g, energy absorption falls below 85%, with significant reductions in both caloric and protein absorption. Furthermore, even without clinically overt diarrhea, increased stool volume may reduce energy absorption, indicating that malabsorption can be underestimated when based solely on symptoms [
13]. These findings support the need for active evaluation of functional digestive and absorptive impairment even in the absence of structural abnormalities.
In this case, recurrent diarrhea, persistent weight loss, and hypoalbuminemia despite the absence of structural abnormalities indicated the need for further evaluation of malabsorption. Ultimately, maintaining adequate nutritional status requires both sufficient nutrient intake and strategies to reduce nutrient loss from impaired absorption.
Fecal elastase testing was a useful noninvasive method for confirming severe EPI in this case. Without structural abnormalities on imaging, this test provided objective confirmation of clinically suspected EPI, such as steatorrhea, and guided important therapeutic decision-making. However, previous studies report that a considerable proportion of patients may have mild or asymptomatic EPI. Therefore, follow-up should include a comprehensive assessment of symptoms such as weight change and laboratory nutritional markers such as serum albumin and micronutrients [
7,
10,
14].
Evidence on PERT after gastrointestinal surgery is limited; however, overall clinical improvements have been reported. Although some studies show no statistically significant symptom improvement, reductions in steatorrhea and improved fat absorption have been consistently reported. These improvements are associated with weight gain, better nutritional status, and improved quality of life [
3-
5].
After confirming severe EPI, pancreatic enzymes were administered with meals, considering the anatomical changes associated with Billroth II reconstruction. Consequently, stool consistency normalized without dietary fat restriction. Improved serum albumin levels and body weight indicated recovery of fat absorption rather than symptomatic management alone.
Routine enzyme supplementation is not required after gastrectomy, but PERT may be effective when clinical symptoms and objective findings indicate EPI. After gastrectomy, reduced gastric acid secretion may impair dissolution and activation of enteric-coated enzyme preparations. Therefore, enzymes should be taken with meals, and opening capsules to mix microspheres with acidic foods may be considered when necessary [
1,
2,
4].
With the increasing number of gastric cancer survivors and an aging population, long-term follow-up will require systematic assessment of nutrition-related complications. In particular, digestive and absorptive dysfunction is expected to become increasingly important clinically. Therefore, persistent diarrhea without obvious structural abnormalities should prompt an integrated nutrition-focused assessment to enable early detection of treatable EPI.
In conclusion, routine PERT is not indicated after gastrectomy, but persistent diarrhea—especially with fat malabsorption—should prompt consideration of EPI as a reversible cause. This case highlights the clinical value of nutrition-focused assessment in detecting malabsorption that conventional diagnostic approaches may miss. With increasing survival rates among patients with gastric cancer and the global trend toward aging populations, periodic and comprehensive nutrition-focused assessment is further emphasized in long-term survivors. Early recognition of EPI and timely PERT initiation with appropriate nutritional intervention can improve gastrointestinal symptoms, nutritional status, and overall outcomes.
NOTES
-
Authors’ contributions
Conceptualization: MK, YK. Data curation: MK. Investigation: SK, MK. Visualization: MK, YK. Writing–original draft: MK, YK. Writing–review & editing: YK, DLJ, SK, JS. All authors read and approved the final manuscript.
-
Conflicts of interest
None.
-
Funding
None.
-
Data availability
Not applicable.
Fig. 1.Mechanisms of fat malabsorption following gastrectomy. (A) Decreased gastric lipase secretion reduces the contribution to initial lipid hydrolysis. (B) Major mechanisms involve anatomical alterations leading to reduced hormonal (CCK, secretin) and neural stimulation, resulting in EPI. Additionally, pancreatobiliary asynchrony impairs the mixing of chyme with enzymes, causing secondary EPI. These factors collectively contribute to fat malabsorption. CCK, cholecystokinin; EPI, exocrine pancreatic insufficiency.
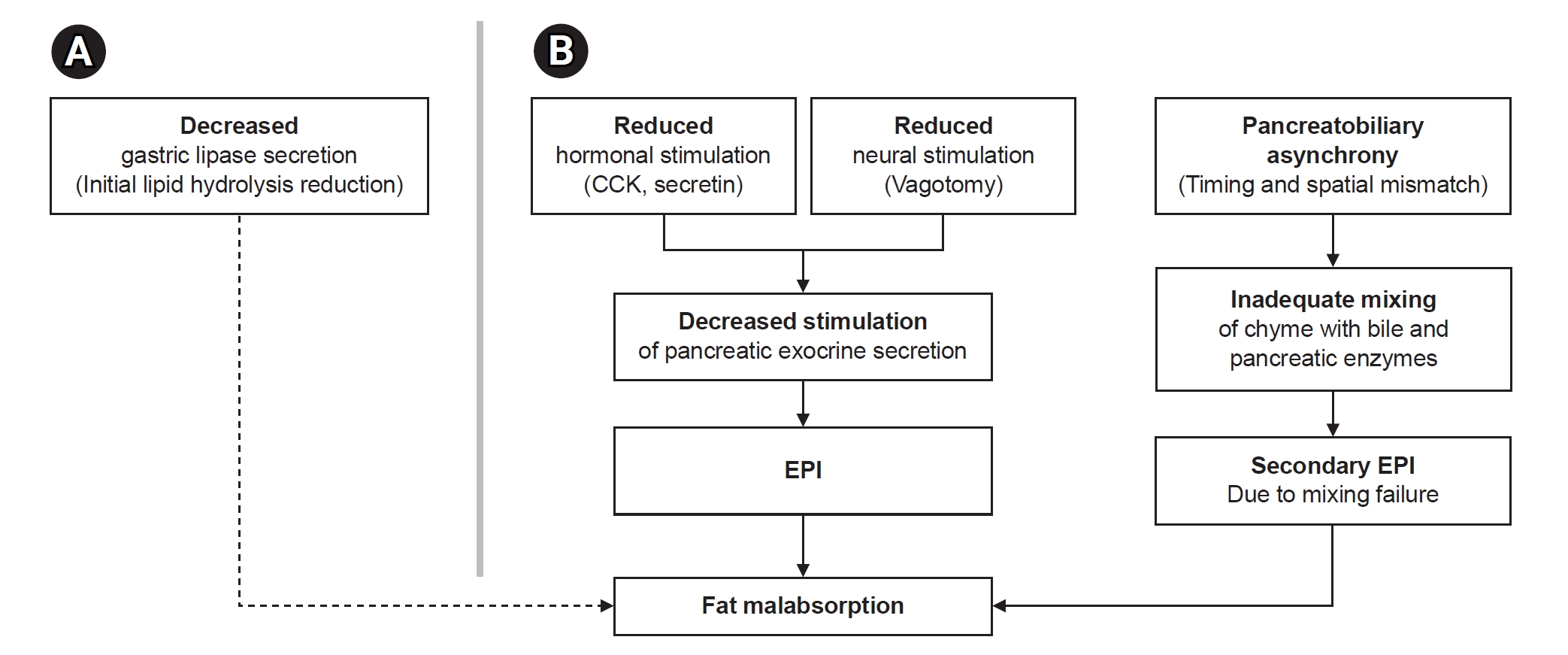
Fig. 2.Clinical course before and after nutritional assessment and PERT. Changes in body weight and serum albumin levels are presented chronologically relative to the initiation of nutritional intervention and PERT. Stool patterns significantly improved from steatorrhea to normal frequency after PERT. PERT, pancreatic enzyme replacement therapy.
REFERENCES
- 1. Dominguez-Munoz JE. Pancreatic enzyme replacement therapy: exocrine pancreatic insufficiency after gastrointestinal surgery. HPB (Oxford) 2009;11 Suppl 3:3-6.
- 2. McVeay C, Davis CA, Thompson SK. Pancreatic insufficiency after gastrectomy: an underdiagnosed condition? ANZ J Surg 2024;94:1674-5.
- 3. Chaudhary A, Dominguez-Munoz JE, Layer P, Lerch MM. Pancreatic exocrine insufficiency as a complication of gastrointestinal surgery and the impact of pancreatic enzyme replacement therapy. Dig Dis 2020;38:53-68.
- 4. Antonini F, Crippa S, Falconi M, Macarri G, Pezzilli R. Pancreatic enzyme replacement therapy after gastric resection: an update. Dig Liver Dis 2018;50:1-5.
- 5. Straatman J, Wiegel J, van der Wielen N, Jansma EP, Cuesta MA, van der Peet DL. Systematic review of exocrine pancreatic insufficiency after gastrectomy for cancer. Dig Surg 2017;34:364-70.
- 6. Blonk L, Wierdsma NJ, Hamer H, et al. Fat malabsorption and reduced exocrine pancreatic function following gastroesophageal cancer surgery. J Gastrointest Surg 2026 Jan 19 [Epub]. https://doi.org/10.1016/j.gassur.2026.102330
- 7. Perbtani Y, Forsmark CE. Update on the diagnosis and management of exocrine pancreatic insufficiency. F1000Res 2019;8:F1000 Faculty Rev-1991.
- 8. Barkin JA, Delk TB, Powell VJ. Symptoms, burden, and unmet needs of patients living with exocrine pancreatic insufficiency: a narrative review of the patient experience. BMC Gastroenterol 2024;24:101.
- 9. de la Iglesia-Garcia D, Vallejo-Senra N, Iglesias-Garcia J, Lopez-Lopez A, Nieto L, Dominguez-Munoz JE. Increased risk of mortality associated with pancreatic exocrine insufficiency in patients with chronic pancreatitis. J Clin Gastroenterol 2018;52:e63-72.
- 10. Dominguez-Munoz JE. Diagnosis and treatment of pancreatic exocrine insufficiency. Curr Opin Gastroenterol 2018;34:349-54.
- 11. Pafumi Y, Lairon D, de la Porte PL, et al. Mechanisms of inhibition of triacylglycerol hydrolysis by human gastric lipase. J Biol Chem 2002;277:28070-9.
- 12. Löhr JM, Panic N, Vujasinovic M, Verbeke CS. The ageing pancreas: a systematic review of the evidence and analysis of the consequences. J Intern Med 2018;283:446-60.
- 13. Wierdsma NJ, Peters JH, Weijs PJ, et al. Malabsorption and nutritional balance in the ICU: fecal weight as a biomarker: a prospective observational pilot study. Crit Care 2011;15:R264.
- 14. Whitcomb DC, Buchner AM, Forsmark CE. AGA clinical practice update on the epidemiology, evaluation, and management of exocrine pancreatic insufficiency: expert review. Gastroenterology 2023;165:1292-301.